Nigeria’s Lassa Fever Outbreak: Risks, Recurrence, Control, and Prevention

It is no longer news that there is an outbreak of Lassa fever in Nigeria; at least the recent case at the University College Hospital (UCH) has drawn attention to this long-standing problem. It is indeed a subject of concern because UCH is a high-risk zone, as infected persons from all over the state may come to receive expert care, thereby exposing healthcare workers and students to risk of infection. That the disease spreads rapidly and is difficult to detect based on symptoms is another cause for alarm. Without effective control, one person exposed could transmit to ten more persons in a few days and so on. Besides, there is no approved vaccine for Lassa fever, meaning it can only be treated (which is only effective with early detection), controlled, and prevented using measures other than vaccination. This startling reality is why we must examine the outbreak, understand the risks, and adopt effective control and preventive measures.
Lassa fever is an acute hemorrhagic illness that is caused by the Lassa virus. The symptoms, which have an onset of 2–21 days post-exposure, typically include fever, weakness, cough, sore throat, headache, muscle pain, nausea, vomiting, and diarrhea. Lassa virus commonly spreads to humans from a rat called Mastomys natalensis, which is endemic in West Africa, common in households, and even eaten as a delicacy in some regions. Once infected, the rat does not become ill but can transmit the virus to humans through contact with its feces and urine throughout its lifetime. Lassa virus may also spread from person to person through direct contact with blood, urine, feces, or other bodily secretions of infected persons. Such transmission is common in healthcare settings with poor infection control. The risk of death from infection is about 1%, but this can climb to as high as 50% during outbreaks. About 15–20% of hospitalized people with Lassa fever die from the disease, while an estimated 80% of infected people are asymptomatic.
The Lassa virus was discovered in 1969 when a missionary nurse, Laura Wine, fell ill with a mysterious disease, which she contracted from an obstetrical patient in Lassa, a village in Borno State, Nigeria. She was then transported to Jos, where she died. Subsequently, two other persons became infected, one of whom was 52-year-old nurse Lily Pinneo, who had cared for Laura Wine. Samples from Pinneo were sent to Yale University in New Haven, where a new virus that would later be known as Lassa virus was isolated for the first time by Jordi Casals-Ariet, Sonja Buckley, and others. Casals contracted the fever and nearly lost his life; one technician died from it. By 1972, the rat, Mastomys natalensis, was found to be the main reservoir of the virus.

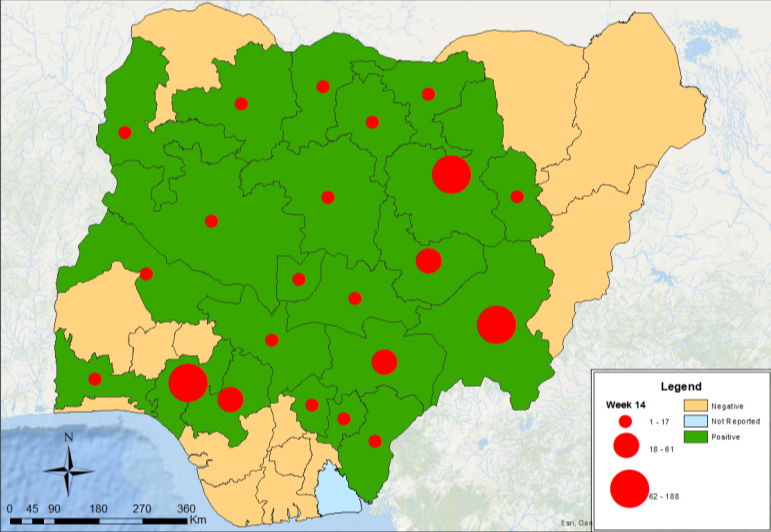
According to the Africa Centers for Disease Control and Prevention, Lassa fever is endemic in West Africa, with an estimated 100,000 to 300,000 cases and over 5,000 deaths occurring annually. The disease is prevalent in Nigeria, Benin, Guinea, Liberia, Sierra Leone, Ghana, and Mali. Nigeria bears the highest burden, with seasonal outbreaks that typically occur during the dry season between December and April. This year, the Nigeria Centre for Disease Control and Prevention (NCDC) has reported a severe outbreak, recording, as of April 5, 2026, a total of 685 confirmed cases, 170 deaths, and a Case Fatality Rate of approximately 24.8%, a significant increase from 18.8% for the same period in 2025. So far, 23 states (including Oyo State) have been affected. 84% of all confirmed Lassa fever cases were reported from five states, including Bauchi (27%), Ondo (22%), Taraba (18%), Edo (9%), and Benue (8%). The latest report from NCDC shows that there are seven suspected cases in Oyo State. However, updated findings from UCH on April 15, 2026, bring the statistics to one confirmed case and death.
The Risks, Control, and Prevention
It is no doubt the ongoing Lassa fever outbreak, particularly the reported incidence at UCH, poses an enormous risk, especially to healthcare workers, patients and their families, and students of the College of Medicine undergoing clinical postings. It is even further worrying that this risk spreads farther to the entire university community, Ibadan, Oyo State, and Nigeria generally. It will, therefore, not come as a surprise if more cases unfold in the coming days. Of course, no one wishes that this should happen, but we can only avoid a catastrophe if we adopt effective control and preventive measures.
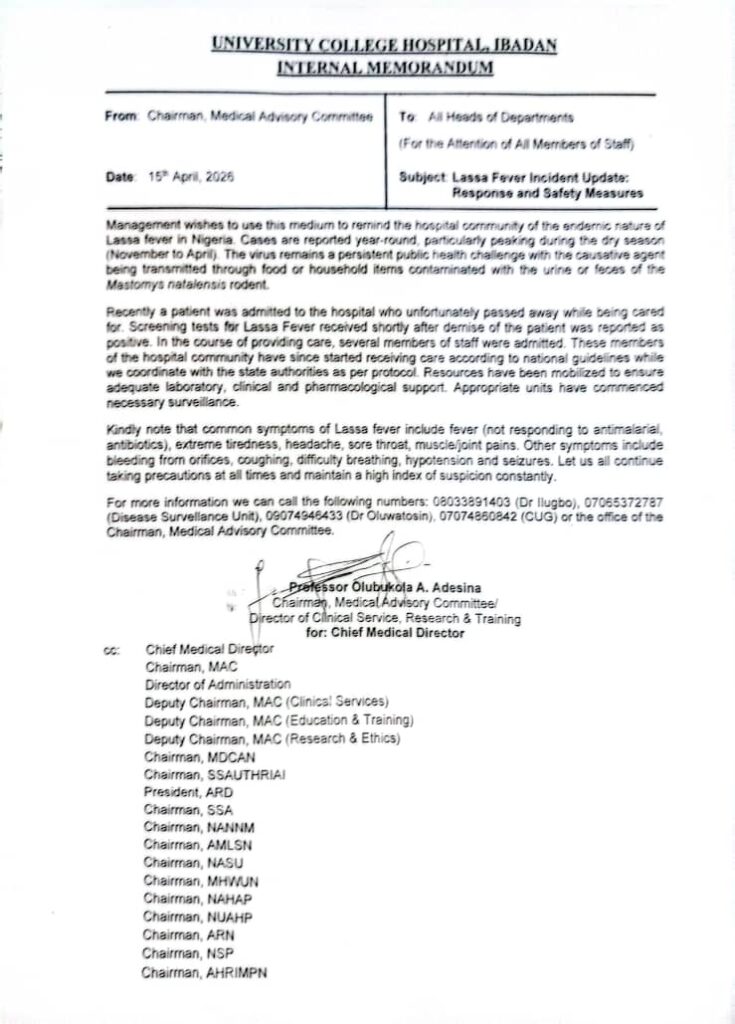
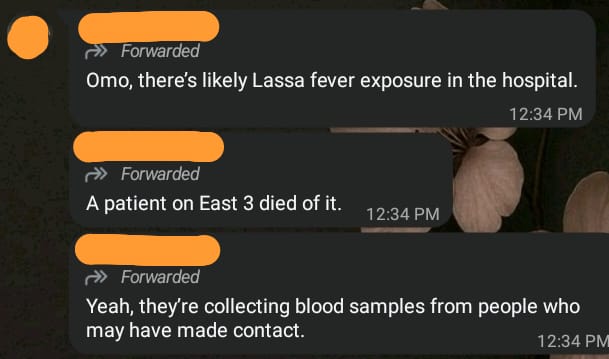
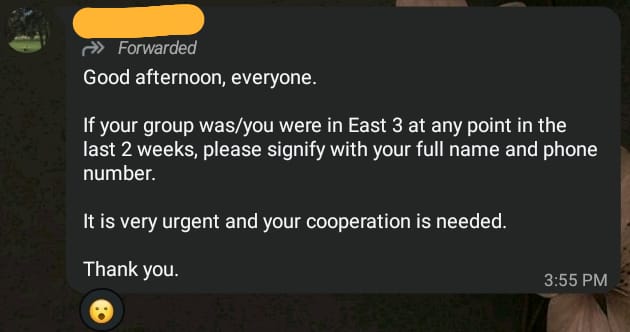
Already, the UCH community has been alerted and active surveillance and contact tracing is ongoing, as revealed in a recent report by the hospital management. According to the report, screening test for Lassa fever for a patient, who unfortunately passed away while receiving care, was reported as positive. In the course of providing care, several members of staff were admitted. Prior to the official report, news about the incidence had begun circulating among students via WhatsApp messages on April 14, 2026.
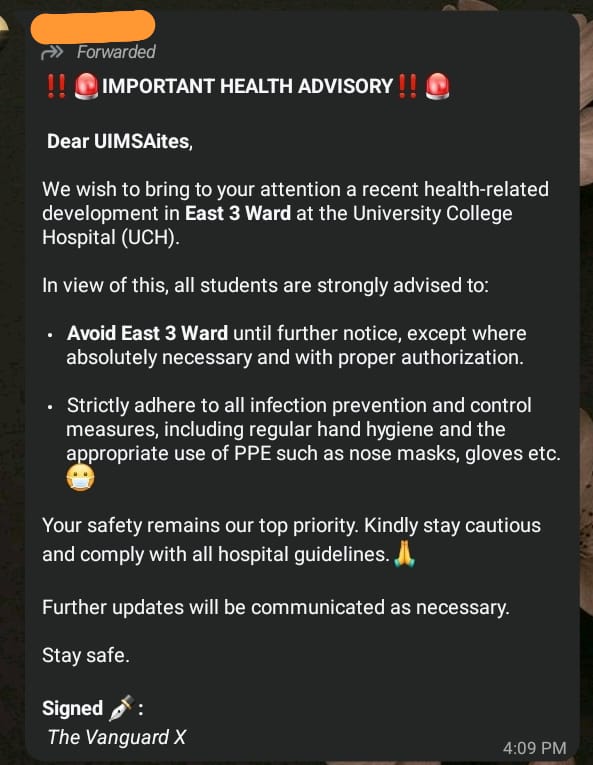
Indeed, everyone must remain vigilant and avoid high-risk zones, especially the hospital ward where the incidence occurred. Anyone who has visited the ward in the past two weeks or suspects symptoms of Lassa fever, either in themselves or others, should promptly notify the Surveillance Unit via 07065372787. Other preventive measures include control of rat infestation, proper sanitation and good personal hygiene, including regular hand hygiene and use of Personal Protective Equipment, such as face masks, gloves, and hand sanitizers.
Unfortunately, there is a rat infestation in Alexander Brown Hall (ABH), where most students of the College of Medicine reside. Some of these rats may be the Mastomys species associated with Lassa fever. This raises concern because the rats would spread Lassa fever at a much faster rate than person-to-person transmission. To alleviate this problem, the health ministers, with the support of the hall management, should declutter gutters and ensure regular weeding and bush clearing within the hall. Students must ensure cleanliness, dispose waste properly, and store food safely. It is our collective responsibility to ensure that Nigeria’s Lassa fever outbreak is effectively controlled.