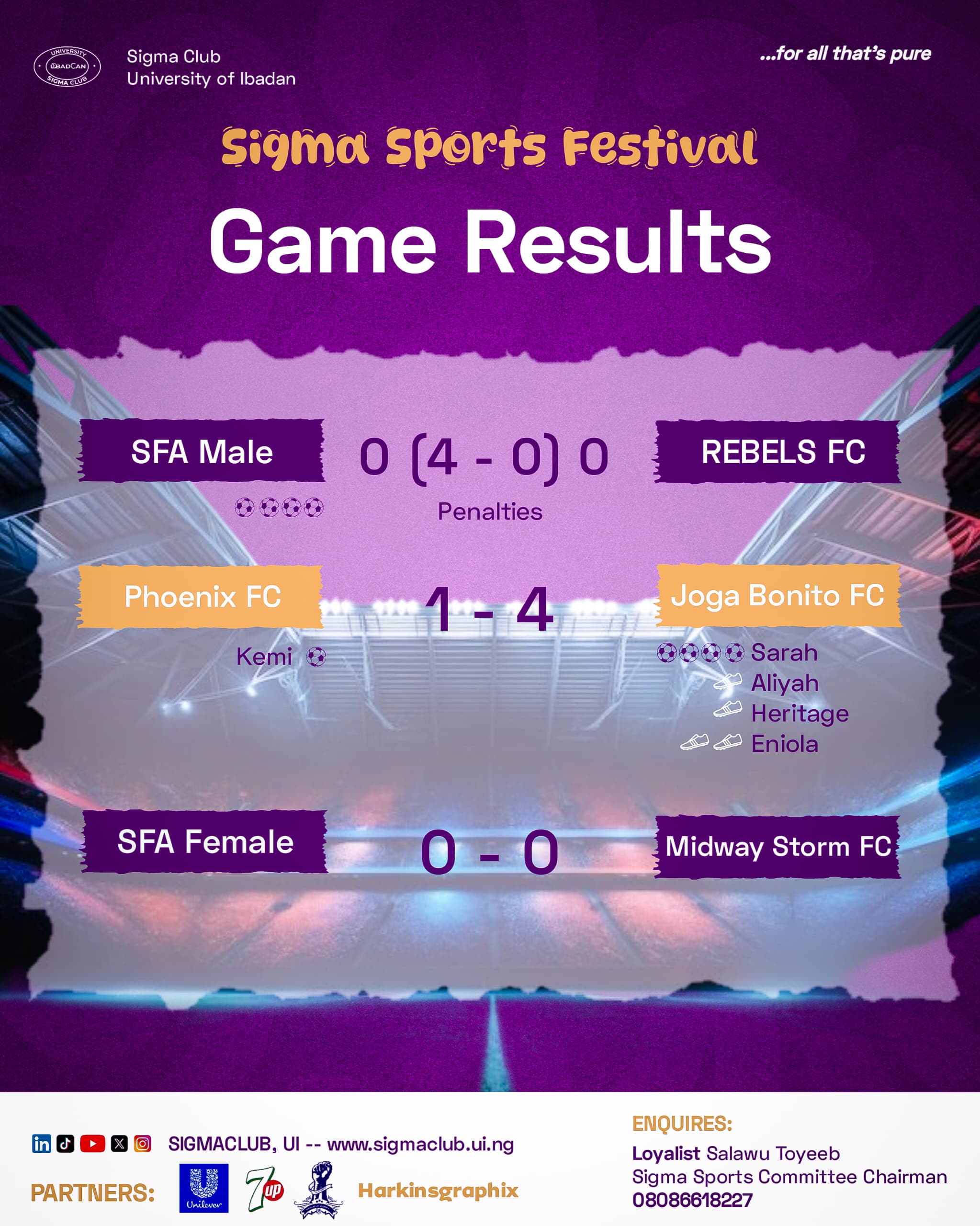
At about 12:30 PM on Friday, September 19, 2025, Soccer For All (SFA) finally kicked off its trophy defense campaign as they faced Rebels FC in a match that, on paper, should have been a walk in the park for SFA. However, Rebels FC held its own against onslaught after onslaught of attacks from SFA. The deadlock remained at the end of the first half, after Korede, SFA’s number 9, missed a 1v1 to break the deadlock. The second half was the other side of the same coin, with Rebel FC’s defense and goalkeeper resilient in shutting out the defending champions. As hopes of an upset began to feel more tangible to the players and supporters of Rebels FC, frustration did the same in the camp of SFA, resulting in Coach Olowu being sent off from the sidelines and skipper Emeka receiving a yellow card in the last moments of added time. The game inevitably progressed to penalty shootouts, where the experience of SFA shone through, putting away all four of their penalties while Rebel FC could not manage to find the back of the net once.

FEMALE CATEGORY
This year’s edition of the Sigma Sports Festival features a female category of football. Five teams registered: SFA (females), Joga Bonito, Phoenix FC, Midway Storm, and Spark Kickers. Because of the number of teams, a league format was decided upon. So, all the teams will play amongst themselves, and then the top 2 teams will progress to the finals.
On Friday, the first game of the female category, Phoenix FC vs. Joga Bonito FC, was held. Although originally billed to be played at Zik Maracana, it was eventually played on the Old SUB Pitch. The first half of the game rained goals, as the Phoenix FC goalkeeper was beaten four different times—all by Sarah!—and the Joga Bonito goalkeeper was beaten just once, by Kemi. The second half was relatively quiet, as both defenses held strong and did not allow any other goals in. The game ended 4-1 in favour of Joga Bonito.

The second game from this category was between SFA and Midway Storm. SFA Femini, in allegiance to their male counterparts, also ended their game in a goalless draw. But because it is in a league format, both teams went home with one point each.
Action returns to the Old SUB Pitch tomorrow, Sunday, the 21st of September, 2025, with the quarterfinals round starting. It features Galacticos FC going against Elite XI by 1:00 PM and Vipers FC facing Forza FC at 2:20 PM.



